See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/295397397
Non-Union Current Treatment Concept
ArticleinShafa Orthopedic Journal · February 2016
DOI: 10.17795/soj-4546
CITATIONS
8
READS
599
3 authors:
Some of the authors of this publication are also working on these related projects:
BCRT, JWI, AG Wildemann View project
Neuroregeneration View project
Arash Moghaddam
Klinikum Aschaffenburg-Alzenau
146 PUBLICATIONS2,057 CITATIONS
SEE PROFILE
Claudia Ermisch
Universität Heidelberg
4 PUBLICATIONS23 CITATIONS
SEE PROFILE
Gerhard Schmidmaier
Universität Heidelberg
265 PUBLICATIONS6,449 CITATIONS
SEE PROFILE
All content following this page was uploaded by Arash Moghaddam on 09 May 2016.
The user has requested enhancement of the downloaded file.

Shafa Ortho J. In Press(InPress):e4546. doi: 10.17795/soj-4546
Published online 2016 February 20. Review Article
Non-Union Current Treatment Concept
Arash Moghaddam,1,* Claudia Ermisch,1 and Gerhard Schmidmaier1
1Center for Orthopedics, Trauma and Spinal Cord Injury, University Hospital Heidelberg, Heidelberg, Germany
*Corresponding author: Arash Moghaddam, Center for Orthopedics, Trauma and Spinal Cord Injury, University Hospital Heidelberg, Heidelberg, Germany. Tel: +49-62215635394, Fax:
+49-62215629123, E-mail: Arash.Moghaddam@med.uni-heidelberg.de
Received 2015 October 31 ; Accepted 2015 December 25.
Abstract
Context: This article wants to give a current concept for the challenging decision for conservative or operative treatment strategies of non-
unions according to the principles of ‘diamond concept’ and aspects that have to be attended.
Evidence Acquisition: Between February 2010 and March 2014, 424 patients with non-unions were treated at Heidelberg university
hospital. This database has been analyzed at least one year after the treatment. The analysis and the experience in surgery and treatment
of non-unions as well as present literature were prepared for this review as a current concept.
Results: If an atrophic non-union is suggested, reosteosynthesis and biological stimulation is required. A revision surgery of autologous
transplantation of cancellous bone from the iliac crest is often enough. Alternatively, reamer-irrigator-aspirator (RIA) can be taken out
of the femur with lower complications and pain in the extraction area and be combined with growth factors like bone morphogenetic
proteins (BMPs), if consolidation after cancellous bone is still absent. In complex cases, consequential and radical removal of the infection
often improved circulation through interventional angiography and use of the two-step procedure (the Masquelet technique) as well as
a tissue covering are required.
Conclusions: By using the ‘diamond concept’ as a complex concept, non-unions can be treated in different stages in a targeted manner.
Keywords: Diamond Concept, Reamer-Irrigator-Aspirator, Non-Union, Masquelet Technique
Copyright © 2016, Iran University of Medical Sciences. This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommer–
cial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/) which permits copy and redistribute the material just in noncommercial usages,
provided the original work is properly cited.
1. Context
The percentage of delayed or non-union after fractures of
long bones is approximately 10%, but depends on patient’s
risk profile. The current definition states that a non-union
is a fracture that will not consolidate without any further
intervention, independent of the treatment time. With
adequate stability, conservative treatment in the early
stages of a non-union is possible. The operative treatment
depends on the type of non-union. There are one-step or
two-step procedures according to the principles of the ‘di–
amond concept’. This involves the improvement of the me–
chanical situation (in most cases with a reosteosynthesis)
and vascularization, local application of osteoconductive
carriers e.g. tricalciumphosphate, vital cells from autolo–
gous bone, and osteoinductive substances like bone mor–
phogenetic proteins (BMP-2 or BMP-7).
Hypertrophic and atrophic non-unions without large
defect gaps or signs of infection can be treated with a
one-step procedure. For treating infected non-unions or
non-unions with large defect gaps, the Masquelet tech-
nique is recommended.
2. Evidence Acquisition
University of Heidelberg hospital is the major center
for orthopaedic treatments in Germany. This database
has been analyzed at least one year after treatment. Our
results were on one hand based on a collective of 424
patients with non-unions who were treated in our cen-
ter between February 2010 and March 2014, and on the
other hand they were based on the current literature on
e.g. PubMed. The analysis and the experience in surgery
and treatment of non-unions as well as present literature
were prepared for this review as a current concept.
3. Results
3.1. Epidemiology
In general, non-union as a complication of fracture
healing occurs in 5% – 10% of cases (1) and can be as high as
30% in high-risk groups (2-5).
The high incidence on the tibia can be explained by poor
tissue covering and therefore poor blood circulation. In ad–
dition, there is more often 2° – 3° of open injuries with com–
plex damage of the bone and the surrounding soft tissue (5).
The incidence of non-unions in bones of the extremi-
ties is as follows: the tibia has on average an occurrence
of 8.7% (6, 7), the femur only slightly less at 6.1% (8-10), the
humerus 3% – 5%, and the lower arm 5% (11-18).
According to the data in our non-union register, there
is a greater presence of non-unions in male patients be-
tween the ages of 30 and 50 years.
Uncorrected Proof

Moghaddam A et al.
Shafa Ortho J. In Press( InPress):e4546
2
3.2. Risk Factors
Besides the type of fracture and the soft tissue damage,
there are other risk factors for the development of non-
unions (19). Smoking increases the risk of delayed heal-
ing or non-unions (5, 20). In addition, advanced age has a
negative effect on physiological fracture healing (21, 22).
Other factors such as diabetes mellitus, the use of non-
steroidal anti-inflammatory drugs (NSAIDs) and previous
fractures of the same extremity also have negative effects
(23, 24). In the risk score according to Moghaddam et al.
all of these risk factors have their relative importance for
measuring the individual risk of a patient for developing
a non-union (5) (Table 1).
3.3. Diagnosis
The diagnosis begins with extensive history taking and
includes the individual risk profile of the patient, taking
into account previous illnesses and medications as well
as all previous conservative and operative treatments.
History of previous infections should be taken into ac-
count as well as the analysis of previous clinical and ra-
diological findings. Blood circulation and soft tissue at
the site of injury should also be evaluated.
Clinical indications of non-union include pain on weight
bearing, limitations to the mobility of an extremity, or in–
stability. In addition, there are clinical signs of infection to
be aware of, such as redness, swelling and warmth or de–
velopment of a fistula. One should especially look out for
local, systemic or anamnestic signs of osteitis.
Conventional radiological imaging of the affected ex-
tremity in two levels with inclusion of joints is standard
for diagnosing faulty positioning or instability. One
should note that defects cannot be completely observed
with native X-rays due to summation and covering. An
additional computed tomography (CT) can be used to
evaluate whether there is partial or entire bridging of the
defect gap. In addition, a contrast magnetic resonance
imaging (MRI) can be used to evaluate vascularization of
the bone and separate vital and non-vital areas (25) (A CT
scan is considered the gold standard for evaluating non-
unions and providing information for treatment).
3.4. Classification
According to the current definition from European society
of tissue regeneration in orthopedics and traumatology (ES–
TROT), a non-union is a fracture that does not heal without
further intervention, independent of the length of treatment.
Non-unions are classically divided into four types: hy-
pertrophic due to mechanical causes, atrophic due to
biological causes, defect, and infection non-unions.
Hypertrophic non-unions develop due to insuffcient
mechanical stability and can lead to formation of a callus
in the area of fracture. Bone consolidation does not occur.
If therapy is delayed, atrophic non-unions can develop
(26). Atrophic non-unions often involve reduced vascu-
larity of the defect gap and surrounding bone, which can
lead to atrophy of the fracture ends. Defect non-unions
usually occur due to high-speed trauma and higher grade
open fractures, which can cause loss of bone through nu-
merous fragments. Furthermore, infected non-unions
develop primarily in open fractures after traumas in
which germs can get into the wound.
Besides the purely morphological classification, there is
a new classification system according to the non-union
scoring system (NUSS) which incorporates bone quality,
soft tissue damage, and the individual patient risk (e.g.
smoking) into a score (27). From this NUSS-score, there
are therapy considerations that can be adapted to the pa-
tient (28-30). The higher the score, the more specialized
and custom the therapy concept must be to offer the pos-
sibility of consolidation (Table 2).
3.5. Therapy
The goal of non-union therapy is the consolidation of bone
defects with correction of the axis and leg length as well as
reaching weight bearing stability. A suffcient tissue covering
as well as removal of the infection are the basic prerequisites.
Independent of the type of non-union and localiza-
tion, therapy can differ in conservative and operative ap-
proaches.
3.5.1. Conservative
Conservative approaches are especially useful in the early
phase of non-union treatment and require suffcient me–
chanical stability as well as bone regeneration potential.
The newest methods in conservative treatment in delayed
fracture healing of the lower extremity are consequential
weight bearing until full weight bearing can be mustered.
The most common methods of conservative treatment in
delayed fracture healing in the area of the lower extremity
are consequential weight bearing to full weight bearing.
Additionally, fractures are treated with daily lower ener-
gy ultrasound (a possibility of conservative therapy is the
application of low energy ultrasound to the defect gap),
over a defined interval of three to six months.
The deciding criteria for successful treatment with low
energy ultrasound are suffcient stability as well as a de-
fect gap of under 10 mm, free of infection in the previous
history, start of therapy in less than five months after the
fracture, and a NUSS-score less than 35 (31).
3.5.2. Operative Treatment Diamond Concept
The multi-factorial causes of delayed fracture healing
make an individual patient’s specific therapy noteworthy.
In this way, the so-called diamond concept (Figure 1) has
become evermore established (3, 32). Therapy consists of
an optimized combination of biological and biomechani–
cal factors (29, 33-38) (The diamond concept has five differ–
ent factors that must be analyzed for therapy) (39).
Non-unions are analyzed according to the following criteria:
– Biomechanical stability; example: through angle sta-
ble implants, dynamized medulla nailing.
Uncorrected Proof

Moghaddam A et al.
– Osteogenic cells: in form of mesenchymal stem cells
(MSCs), autologous cancellous bone (iliac crest or reamer
irrigator aspirator (RIA)).
– Osteoconductive structures; example: autologous can-
cellous bone, synthetic bone replacement material (ex-
ample: tricalcium phosphate).
– Growth hormones; examples: bone morphogenetic
protein (BMP)-2 and BMP-7.
– Vascularization: through improving the macro-circu-
lation and local induction of a Masquelet membrane re-
newal of the fracture ends.
In looking at individual clinical and radiological param-
eters, there are a number of factors lacking in a combi-
nation treatment and therefore, systemic optimization
of the biological and biomechanical treatment of non-
unions should be looked at (29, 34, 40, 41).
3.5.3. Isolation of Bone Replacement Material
The iliac crest often serves as the source of autologous
cancellous bone. The method involved is widely used and
is considered the gold standard in the surgical treatment
of non-unions. It has the optimal consistency and can es–
tablish good primary stability as a tricortical graft. Prob–
lematic is the limited availability and differing quality and
quantity as well as a high extraction morbidity (25, 42-46).
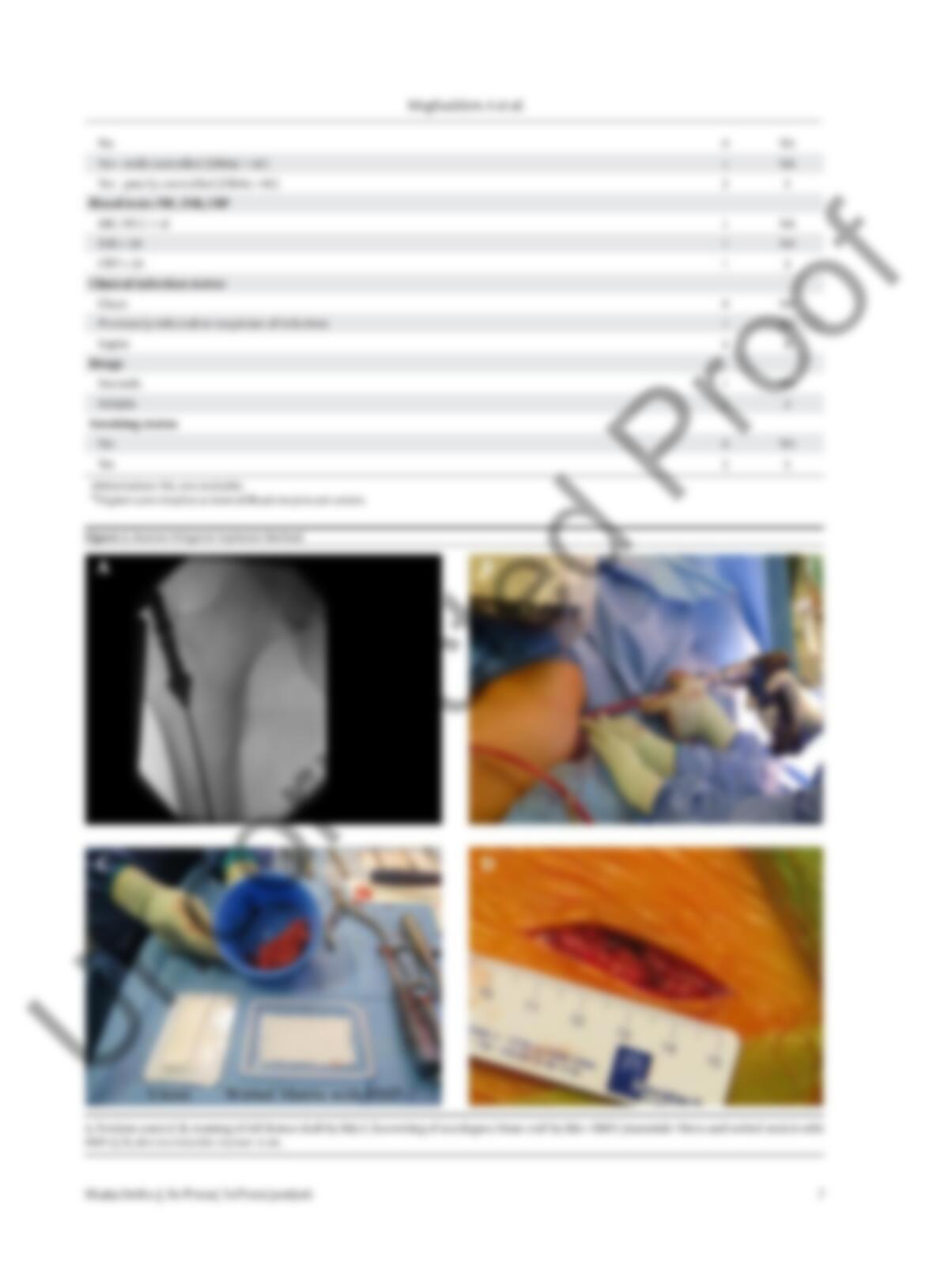
An alternative to autologous cancellous bone extraction
is the use of RIA (Depuy-Synthes, USA) (Figure 2). In this
procedure, the percutaneous opening of the medullary
cavity is performed with a combination of drilling, clean–
ing and vacuum extraction of MSCs out of long bones. This
method is primarily performed on the femur, but can also
be done on the tibia. In this way, it is possible to extract 80
cm of the autologous bone material for transplantation
ture healing and bone regeneration. Currently, there are
two growth hormones permitted for use in orthopedics
and trauma surgery. These include BMP 2 for open lower
leg fractures and BMP-7 for non-unions of the tibia.
Studies over the past years have shown that the use of
BMP-7 is at least equal to a single cancellous bone graft (52).
Furthermore, there are adequate indications in everyday
clinical routine to suggest increases in the healing rate of
non-unions (18). The combination of autologous cancellous
bone with BMPs is clearly superior to a single cancellous
bone graft (53).
BMP-7 is not currently commercially available; so, increased
BMP-2 (Medtronic) can be used in non-union therapy.
The authors recommend the additional use of BMPs in a
failed therapy with autologous cancellous bone. In addi–
tion, when the effect is clearly proven by clinical studies, we
recommend receiving approval of costs from the insurance
company and approval of its use from a panel of experts.
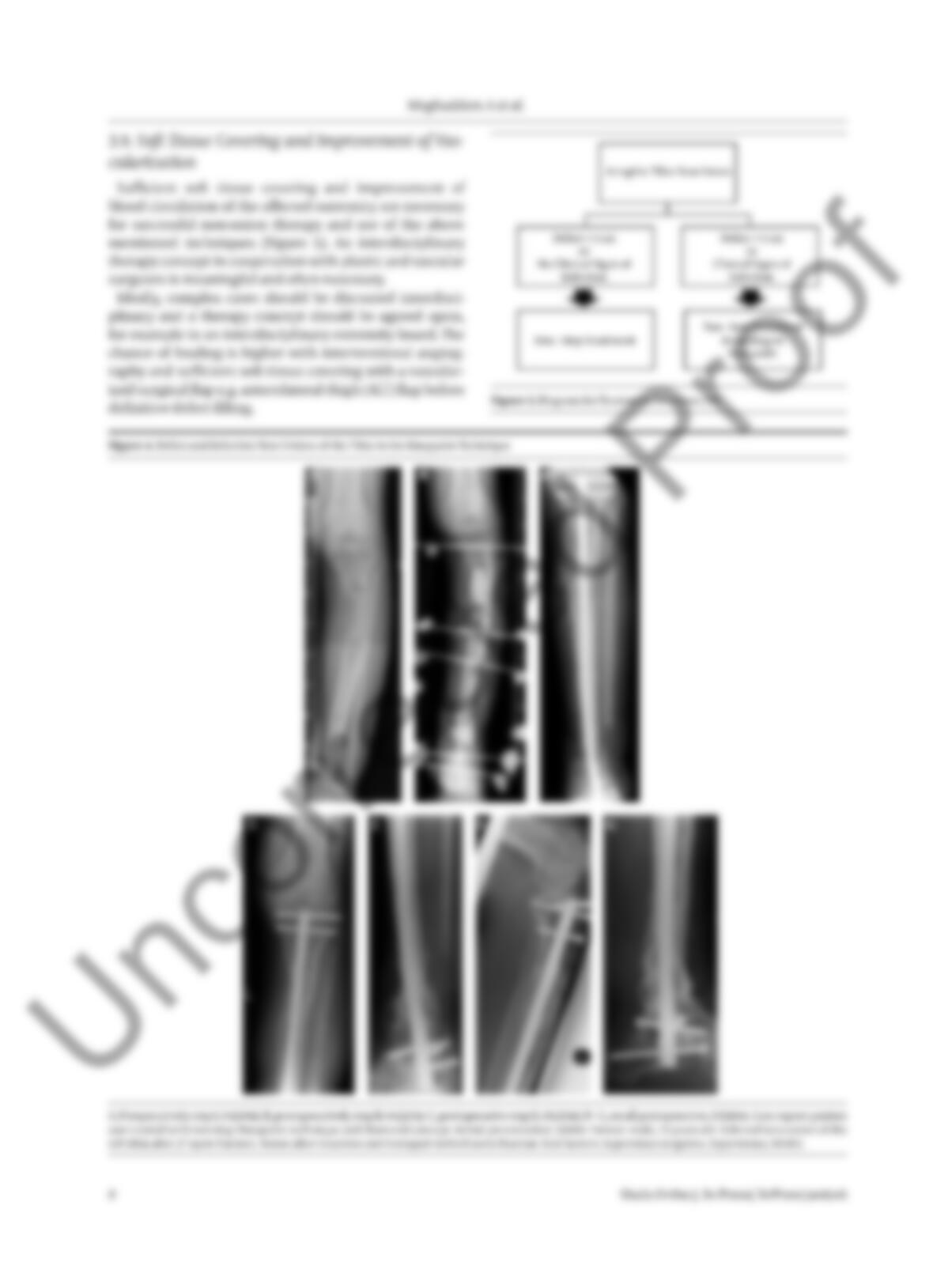
3.6. Bone Marrow Drilling in Hypertrophic Non-
Unions
According to the diamond concept, optimizing mechani–
cal stability is indicated in hypertrophic non-unions. In the
case of an instable osteosynthesis, a reosteosynthesis is nec–
essary. In simple cases, the dynamization of an adjoining
nail with full weight bearing is possible. In complex cases, a
reosteosynthesis with medullary cavity drilling and medul–
lary nail osteosynthesis with a thick nail is necessary (54) (in
hypertrophic non-unions in the tibia shaft area, medullary
cavity drilling and nail osteosynthesis has been indicated).
3.6.1. Positioning
A patient is positioned on the back and the x-ray beam is po–