Communication skills
• Open and closed questions:
➢ Open questions are responded to with a wide range of non-specific answers.
➢ Closed questions are responded to with a narrow range of specific answers.
• Screening:
➢ Asking the patient if they have other complaints.
• Negotiation of agenda:
➢ Deciding on the chief complaint.
➢ Involving the patient in the decision.
• Active listening:
➢ Paying attention as the patient talks.
➢ Not interrupting the patient.
➢ Giving the patient encouraging signs as to continue talking (e.g., go on, I see… etc.).
• Facilitative response:
➢ Giving the patient the appropriate response after actively listening to what they have to say.
• Clarification:
➢ Making sure that the patient understands you, and you them.
➢ Knowing the characteristics of diseases (requires previous knowledge, plus information acquired from
the patient).
• Signposting:
➢ Giving the patient a heads-up about what you are going to ask next.
• Developing rapport:
➢ Breaking the ice between the patient and yourself.
➢ To avoid “white-coat syndrome” (people’s fear of doctors as they fear bad news of bearing illness and
whatnot).
➢ To avoid “white–coat hypertension” (increase in blood pressure of the patient when they say doctors).
• Establish the sequence of events:
➢ In order to make sure that you have asked all the required questions.
➢ To make sure that you have arranged the events in the correct chronological order.
• Clear language:
➢ Not using technical terms.
➢ Speak in a language that the patient would easily understand.
• Empathy:
➢ Make the patient feel that you relate to them.
➢ Does not involve judgment.
➢ Does not involve giving unacquired advice.
• Sympathy:
➢ Understanding from your own perspective.
➢ Involves a lot of judgment.
➢ Involves giving unacquired advice.
• Involving the patient:
➢ Explaining the procedures to be done.
➢ See if the patient is capable of doing necessary procedures (financially, socially…etc.)
History Taking
Introduction,
patient’s
profile
Presenting
complaint(s)
History of
presenting
complaints
Patients
perspective Medical and
surgical history
Family history
Drug history
and allergies
Social history
Summary
1. Introduction, patient’s profile:
➢ Maintain patient’s privacy.
➢ Sanitize your hands.
➢ Introduce yourself.
➢ Greet the patient.
➢ Ask the patient if they would like to have a chaperone.
➢ Acquire consent from the patient to take their history.
➢ Acquire patient’s profile:
▪ Name.
▪ Age.
▪ Gender.
▪ Occupation.
▪ Marital status/children.
2. Presenting complaint:
➢ Ask the patient why did they come to see you.
➢ Ask the patient if they have any other complaints
➢ Negotiate the agenda with the patient, and decide on the chief complaint.
3. History of presenting complaints:
➢ “Story of symptoms”.
➢ Establish the sequence of events.
➢ For pain use SOCRATES.
1) Site; where is the pain.
2) Onset; when did the pain start.
3) Character; how does the pain feel like.
4) Radiation; does the pain spread.
5) Associated symptoms.
6) Timing; is the pain continuous or episodic, and does it occur during the day or at night.
7) Exacerbating and relieving factors.
8) Severity; on a scale of 1 to 10, how bad is the pain.
➢ If the patient has something other than pain (e.g., nausea), use OCATES (See the list above).
4. Patient’s perspective:
➢ Find out what the patient thinks or feels about their symptoms.
➢ Use ICE:
1) Ideas.
2) Concerns.
3) Expectations.
➢ Or use FIFE:
1) Feelings.
2) Ideas.
3) Function.
4) Expectations.
5. Past medical and surgical history:
➢ Does the patient have any current or past medical problems (e.g., any chronic diseases)?
➢ Did the patient have any previous visits to the doctor or hospital, and what was the cause?
➢ Did the patient have any previous surgeries? (What was the surgery, why did they have it, where did
they have it, how much time did they spend as in-patients, did they suffer from any post-surgical
complications).
6. Family history:
➢ When suspecting genetic disorders:
▪ Document 3 family generations in pedigree diagram.
▪ Acquire information about the patient’s parents (alive or dead, any chronic diseases, cancers,
inherited diseases, or autoimmune diseases that they have or have had).
7. Drug history and allergies:
➢ Is the patient currently taking any drugs? (Why, what does, how much, since when, for how long, is the
patient committed to taking the drug).
➢ Does the patient have any drug allergies?
8. Social history:
➢ Does the patient smoke (how much, have they ever smoked, when was the last time they did smoke)?
➢ Does the patient drink alcohol?
➢ Is the patient subject to drug abuse?
➢ Did the patient travel anywhere recently?
➢ Is there anything the patient would like to add about, for example, their childhood experience, current
and past relationships, lifestyle factors?
9. Summary.
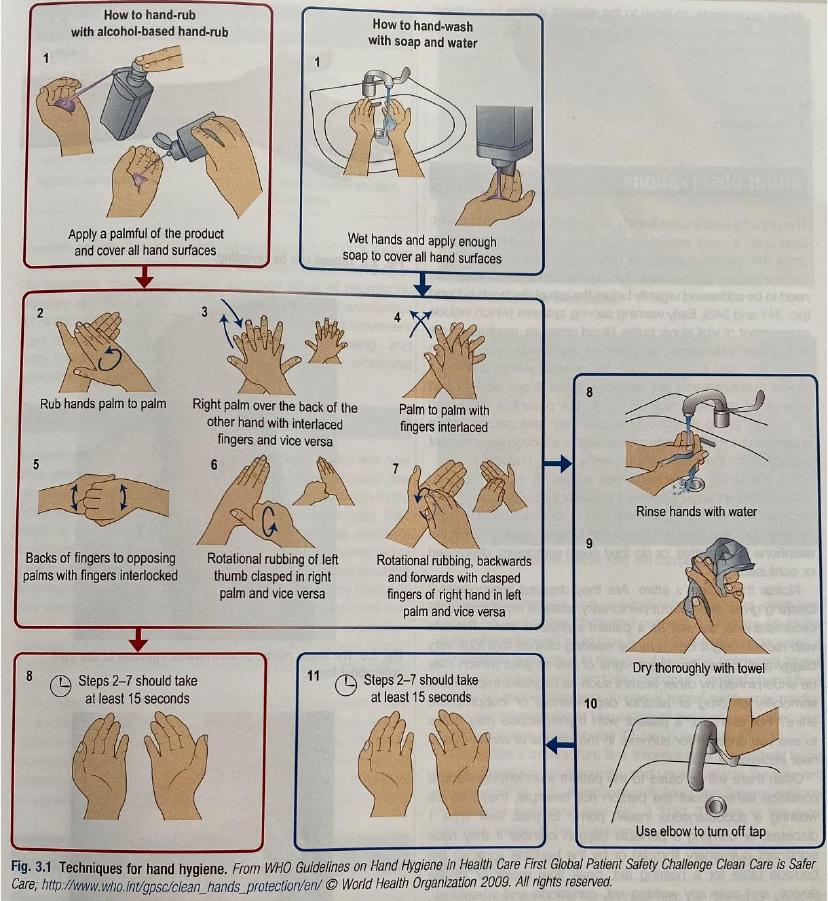
Hand Washing Technique
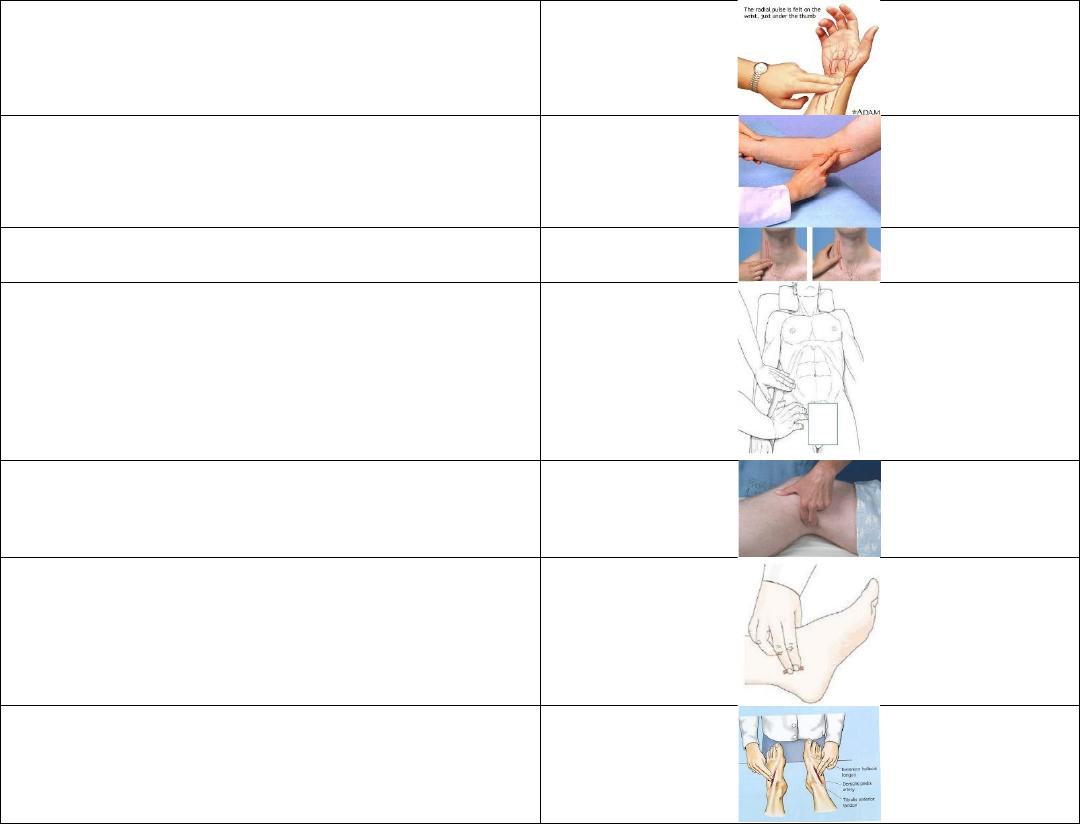
Palpable Arteries
Radial
Brachial
Carotid
Femoral
Popliteal
Posterior Tibial
Dorsalis Pedis

Physical Examination
▪ Physical examination starts as soon as you see the patient.
▪ Vital points during physical examination:
1. Maintain patient’s privacy.
2. Acquire patient’s consent.
3. Maintain professionalism.
➢ Professionalism: knowing what to do, how to do it, and when to do it.
➢ Professional: a person who can do their best work at all times, regardless of how they feel.
▪ General examination sequence when examining any part of the body:
1. Inspection: look.
2. Palpation: touch.
3. Percussion: tap.














